|
|
Clinical Cases |
|
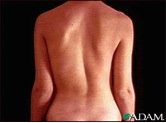
Scoliosis
Scoliosis is a medical condition in which the spine undergoes abnormal lateral and/or rotational curvature. The typical spine is laterally straight with an S-shaped anterior-posterior curve (the cervical and lumbar spine exhibit slight lordosis- anterior convexity- and the thoracic and sacral spine exhibit slight kyphosis- posterior convexity). Scoliosis patients have spines that curve laterally, creating a C or S shape to the spine when viewed from the patient’s back. Most cases of scoliosis are idiopathic (unknown cause). These cases are classified into 3 types based on the age of the patient when scoliosis develops:
- If the patient is less than 3 years old they have infantile idiopathic scoliosis.
- 3-10 years old is juvenile idiopathic scoliosis.
- Greater than 10 years old is adolescent idiopathic scoliosis.
There are three types of scoliosis with known etiology:
- Functional scoliosis develops due to a mechanical problem such as one leg being shorter than the other.
- Neuromuscular scoliosis is the result of abnormal spine development such as spina bifida occulta.
- Degenerative scoliosis typically occurs in old age and is the result of arthritic weakening of the spine.
Scoliosis is a relatively common condition. The majority of individuals with scoliosis do not require surgery or braces because their condition is self-limiting. Progressive scoliosis, however, requires therapy.
The image shown here is the scout film of cadaver 33448. Notice how the spine has a slight C-shaped curve involving the lower thoracic and lumbar vertebrae. The curve is convex toward the patient's left.
The movie shown here is a CT scan of the same cadaver. The cervical spine can be found at time= 40-45, K8. Advance the movie forward (moving the cross section further down the body) while following the spine. The transition from cervical spine to thoracic spine occurs at time= 48. This transition is marked by the appearance of the 1st and 2nd ribs coming off of the T1 and T2 vertebrae. Continue keeping track of your level on the spine by counting ribs as they come off the vertebrae as you advance the movie forward. Notice that around T10, time= 60, the spine begins shifting to the patient's left (remember: the orientation of CT scans places the viewer at the foot of the patient looking toward the head, so the patient's left is on the viewer's right). From T10- L5 the spinal column is seen to deviate to the left and then come back to center just as the iliac crests come into view. You will also notice that the spinal column moves anteriorly while viewing L1-L5; this is normal lordotic curving of the lumbar spine.
Consequences of Scoliosis
The prognosis for scoliosis depends on the severity of curvature and degree of skeletal maturity upon onset. When taken together, these two factors help predict the likelihood of progressive scoliosis, and so can direct the clinician to the appropriate course of action.
Severe scoliosis can cause a variety of health problems ranging from musculoskeletal to cardiopulmonary dysfunction. A severe scoliosis of the thoracic spine can lead to diminished lung volume (or hypoplastic lung if the curve obstructs the thoracic cavity during lung growth) and can sometimes cause heart problems due to the spine putting direct pressure on the heart.
This child’s scoliosis is clearly obstructing his/her right chest cavity. Lung development and volume will be mechanically inhibited.

Treatment
- Wait and observe the spine at regular intervals to determine if the curvature is worsening.
- Physiotherapy - This treatment method is based on the idea that scoliosis results from a complex array of muscular asymmetries. Specialists create exercise regimens for patients that are designed to correct these asymmetries.
- Occupational therapy to help the patient manage their symptoms so that they can maximize their quality of life (a palliative, rather than curative or preventive, treatment option)
- Bracing - This method is best for patients who still have bone growth remaining. It is not capable of correcting a curve, only impeding the progression of the curve. Braces are typically worn 22-24 hours per day, and their effectiveness depends on both the fit of the brace and patient compliance.

- Surgery is typically indicated in curves of greater than 45-50 degrees that have a likelihood of progression, curves in patients with spina bifida and cerebral palsy, and curves that affect physiologic function (such as those that inhibit lung expansion and put pressure on the heart). A number of surgical procedures have been developed to correct scoliosis. Modern spinal surgeries use mechanical systems of rods, screws, hooks and wires to correct both lateral and rotational defects.
Thoracic dextroscoliosis (convexity to the right)
and lumbar levoscoliosis (convexity to the left).
This X-ray was taken with the patient laying face down.Same patient after corrective surgery. This is the scout film and CT scan of cadaver 33486, which shows a case of thoracic levoscoliosis (left convexity) and lumbar dextroscoliosis (right convexity). Look first at the anterior-posterior scout film to appreciate the curvature and make reference of where the major curves are, then look at the CT scan and watch the spine curve first to the left then the right as you scan from thoracic to lumbar vertebrae.